2026-03-09 14:39 Tags:Technical Literacy
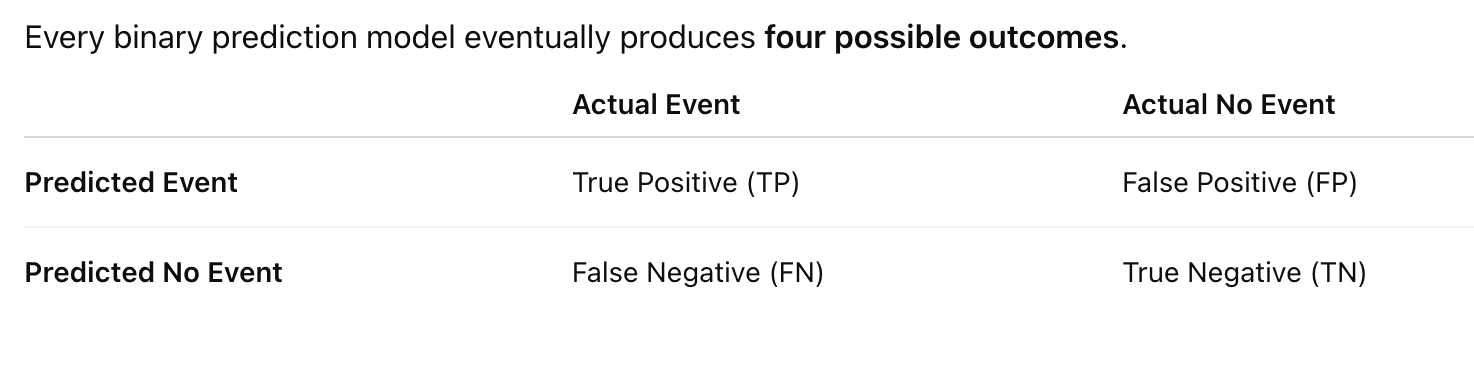
1. Start With the Confusion Matrix
| Case | Model Prediction | Actual Outcome |
|---|---|---|
| Patient A | High risk | Adverse outcome |
| Patient B | High risk | No event |
| Patient C | Low risk | Adverse outcome |
| Patient D | Low risk | No event |
So we get:
TP = predicted event and event happens
FP = predicted event but no event happens
FN = predicted no event but event happens
TN = predicted no event and no event happens
2. Recall (Sensitivity)
Recall answers this question:
Among all patients who actually had adverse outcomes, how many did the model detect?
Formula:
Recall = TP / (TP + FN)
Example:
Suppose in your dataset:
Total real adverse outcomes = 100
Model detected = 60
Missed = 40
Then
Recall = 60 / 100 = 0.60
Meaning:
The model catches 60% of dangerous cases.
Why Recall Matters in Healthcare
Missing a dangerous patient can be very costly.
Example:
Patient refuses transport
Model says low risk
Patient deteriorates later
So many medical systems prefer:
Higher recall
Even if it means more false alarms.
3. Precision
Precision answers a different question:
Among patients predicted as high risk, how many actually have events?
Formula:
Precision = TP / (TP + FP)
Example:
Model flags:
100 high-risk patients
But only:
20 actually have adverse outcomes
Then
Precision = 20 / 100 = 0.20
Meaning:
Only 20% of alerts are real events.
4. Why Precision Matters
Too many false alarms can overwhelm the system.
Example EMS scenario:
Model flags 500 patients
But only 20 truly deteriorate
Clinicians will stop trusting the system.
So precision controls alert quality.
5. Precision vs Recall Trade-off
Usually you cannot maximize both.
Example threshold:
Risk > 0.20 → high risk
Model flags many patients.
Result:
Recall ↑
Precision ↓
Lower threshold catches more events but produces more false positives.
If you increase threshold:
Risk > 0.60 → high risk
Now only extreme patients flagged.
Result:
Precision ↑
Recall ↓
You catch fewer events but alerts are more accurate.
6. Intuition With Your EMS Project
Imagine:
10,000 refusal patients
100 adverse outcomes
Model flags top 500 high-risk patients.
Among them:
50 events
Then
Precision = 50 / 500 = 10%
Recall = 50 / 100 = 50%
Interpretation:
Half of dangerous patients are detected
But 90% of alerts are false alarms
This is actually very common in rare event prediction.
7. Why Precision/Recall Matters More Than Accuracy
Accuracy:
(TP + TN) / Total
In rare events this is misleading.
Example:
Event rate = 1%
If model predicts:
No event for everyone
Accuracy:
99%
But recall:
0%
Model is useless.
8. Precision-Recall Curve
Instead of picking one threshold, we can evaluate all thresholds.
Plot:
Recall (x-axis)
Precision (y-axis)
This gives a PR curve.
Area under this curve:
Average Precision
This metric is better than ROC when events are rare.
Many healthcare ML papers report both.
9. Relationship With AUC
They measure different things.
| Metric | Meaning |
|---|---|
| AUC | ranking ability |
| Precision | quality of positive predictions |
| Recall | ability to detect events |
So a model can have:
Good AUC
Poor precision
Especially when events are rare.
11. A Small Mental Model
Think of it like this:
Recall → How many dangerous patients we catch
Precision → How reliable our alerts are
Both matter depending on the clinical objective.
Recall = Sensitivity
Precision ≠ Specificity
So only one pair is the same.
1. Recall = Sensitivity (Correct)
These two are the same metric, just used in different fields.
In machine learning we say Recall.
In medicine we say Sensitivity.
Formula:
[
Recall = Sensitivity = \frac{TP}{TP + FN}
]
Meaning:
Among all real events, how many did we detect?
Example in your EMS model:
If 100 patients truly deteriorate and your model detects 60:
Recall / Sensitivity = 60%
So:
Recall = Sensitivity
2. Specificity (Different from Precision)
Specificity measures something different.
Formula:
[
Specificity = \frac{TN}{TN + FP}
]
Meaning:
Among patients without events, how many did we correctly identify as safe?
Example:
If 9900 patients have no adverse outcome and the model correctly predicts 9800 as safe:
Specificity = 9800 / 9900
3. Precision (Different concept)
Precision focuses on the predicted positives.
Formula:
Meaning:
Among predicted high-risk patients, how many actually have events?
Example:
Model flags 100 high-risk patients.
If 30 actually deteriorate:
Precision = 30 / 100 = 30%
4. Visual Comparison (Very Helpful)
| Metric | Formula | Question it answers |
|---|---|---|
| Sensitivity / Recall | TP / (TP + FN) | Did we catch the events? |
| Specificity | TN / (TN + FP) | Did we correctly identify safe patients? |
| Precision | TP / (TP + FP) | Are our alerts correct? |
5. Why Precision and Specificity Feel Similar
They both involve false positives, which causes confusion.
But they answer different questions.
Specificity asks:
Among actual negatives, how many are correctly predicted?
Precision asks:
Among predicted positives, how many are correct?
Different denominators.
6. Simple EMS Example
Imagine:
10,000 refusal patients
100 adverse outcomes
Model results:
TP = 50
FP = 150
FN = 50
TN = 9750
Now compute:
Recall / Sensitivity:
50 / (50 + 50) = 50%
Specificity:
9750 / (9750 + 150) ≈ 98.5%
Precision:
50 / (50 + 150) = 25%
Interpretation:
-
Model catches half the dangerous patients
-
Correctly identifies almost all safe patients
-
Only 25% of alerts are real
This pattern is very common in rare-event prediction.
7. The Key Mental Model
Think of it like this:
Sensitivity / Recall → detect dangerous patients
Specificity → identify safe patients
Precision → how trustworthy our alerts are
Each metric answers a different clinical question.
8. One Small Trick to Remember
Look at the denominator.
Recall / Sensitivity:
TP + FN
→ all actual positives
Precision:
TP + FP
→ all predicted positives
Specificity:
TN + FP
→ all actual negatives